IMCIVREE delivered early, significant, and sustained weight reduction1,2
BMI Z-score* reduction in patients 6 to <18 years of age1-3†
In patients 6 to <18 years of age with BBS
IMCIVREE significantly reduced weight1
Weight changes in pivotal and supplemental patients 6 to <18 years of age with BBS during the 14-week double‑blind, placebo-controlled period1*
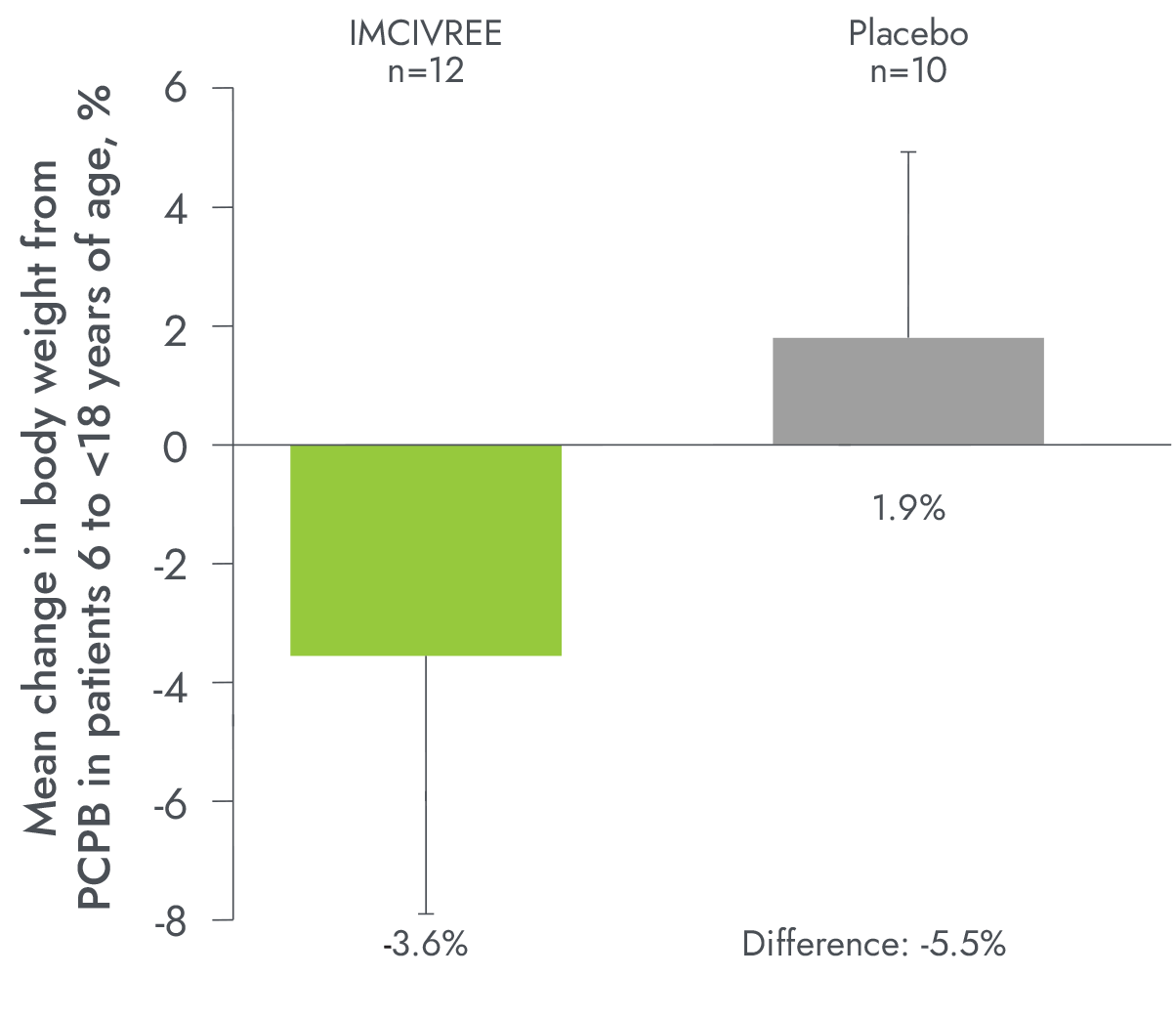
*Results in sub-population based on post-hoc analysis. Supplemental patients were enrolled after the pivotal cohort had begun treatment. None of the supplemental patients had completed 52 weeks of IMCIVREE treatment at the time of data analysis.1
PCPB=placebo-controlled period baseline.
Reference: 1. Haqq AM et al. Lancet Diabetes Endocrinol. 2022;10(12):859-868. doi:10.1016/S2213-8587(22)00277-7. Supplemental appendix available at: https://www.thelancet.com/journals/landia/article/PIIS2213-8587(22)00277-7/fulltext.
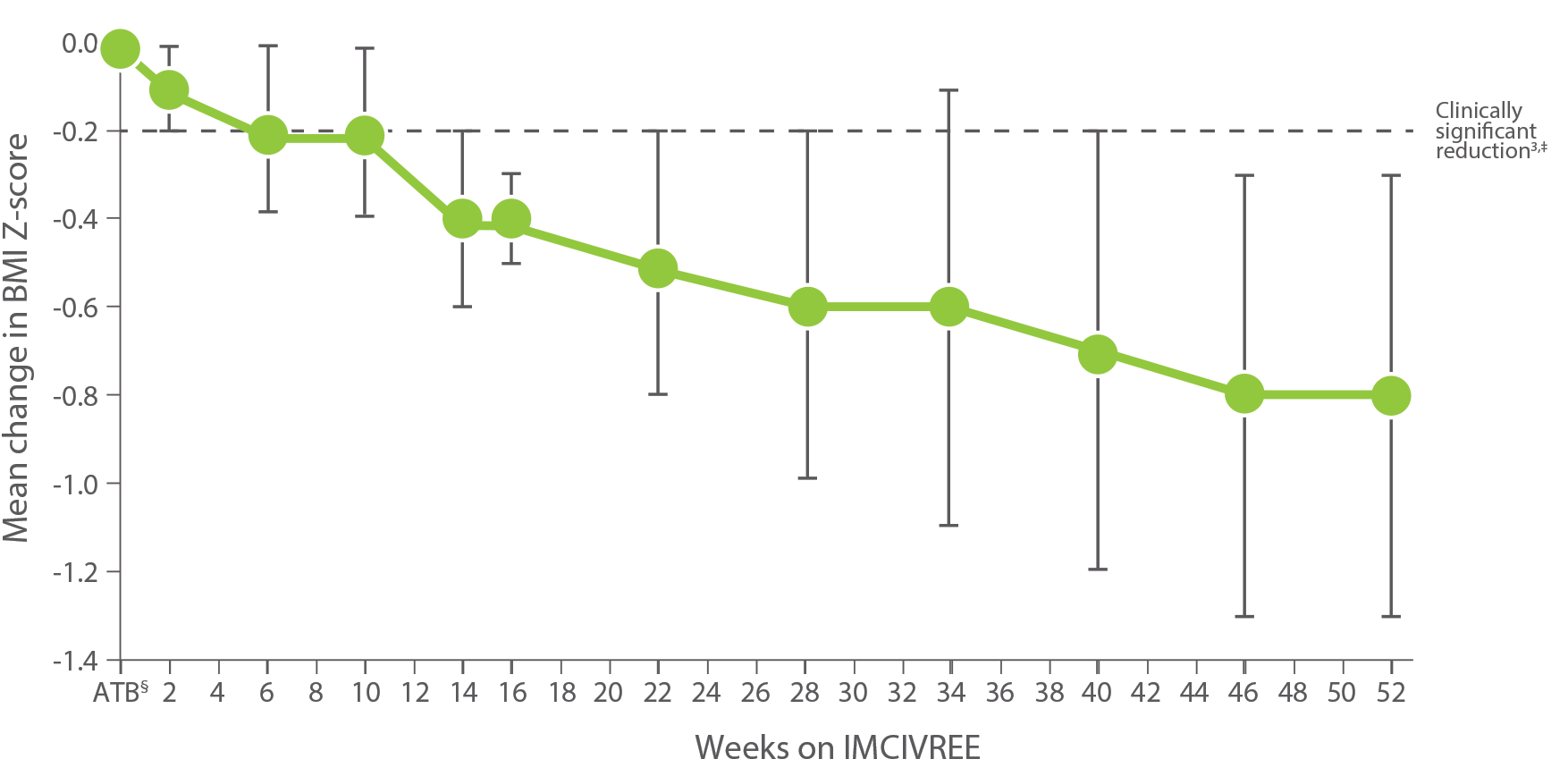
Clinically significant -0.8 mean change in BMI Z-score at week 521,2
- Sustained mean reductions in BMI Z-score at 24 months in a long-term extension study4
*BMI Z-score was an exploratory endpoint used to measure the reduction in BMI in children. A BMI Z-score is a reliable measure of weight in children who are still growing because it accounts for height, age, and gender.1,5
†Data shown include only patients who received 52 weeks of IMCIVREE at the time of the analysis. Population sizes ranged from 8 to 16, with n=14 at 52 weeks on active treatment. Error bars are the standard deviation.1
‡A clinically significant reduction is generally considered a ≥0.2 reduction in BMI Z-score. A 0.2 reduction is comparable to weight loss of approximately 5%.2
§ATB=active treatment baseline, defined as the last measurement before the first dose of IMCIVREE; ie, week 0 for IMCIVREE group and week 14 for placebo group.1
Change in BMI Z-score from baseline in patients 6 to <18 years of age after 52 weeks (n=14)3
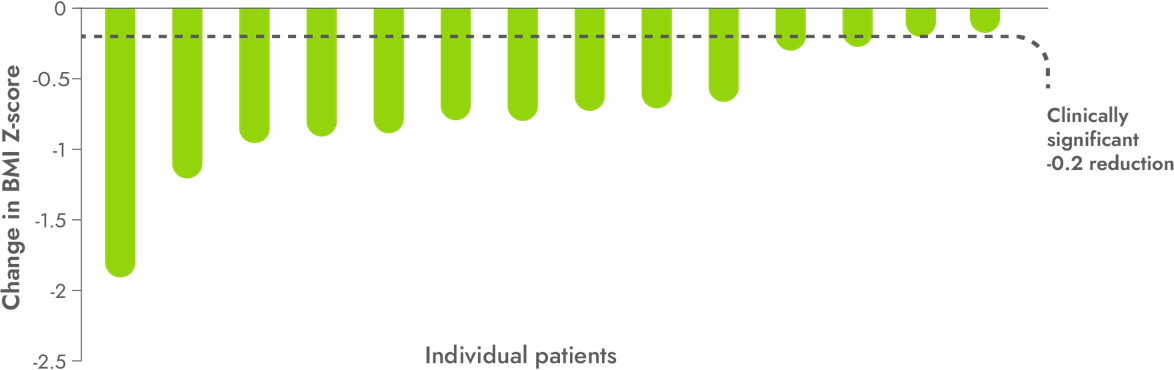
86%
of patients achieved a clinically significant ≥0.2 mean reduction* in BMI Z-score1,3
- 100% of patients 6 to <12 years of age achieved a clinically significant ≥0.2 reduction in BMI Z-score (n=3)
In patients 6 to <18 years of age with BBS
IMCIVREE significantly reduced weight1
Weight changes in pivotal and supplemental patients 6 to <18 years of age with BBS during the 14-week double‑blind, placebo-controlled period1*
*Results in sub-population based on post-hoc analysis. Supplemental patients were enrolled after the pivotal cohort had begun treatment. None of the supplemental patients had completed 52 weeks of IMCIVREE treatment at the time of data analysis.1
PCPB=placebo-controlled period baseline.
Reference: 1. Haqq AM et al. Lancet Diabetes Endocrinol. 2022;10(12):859-868. doi:10.1016/S2213-8587(22)00277-7. Supplemental appendix available at: https://www.thelancet.com/journals/landia/article/PIIS2213-8587(22)00277-7/fulltext.
*BMI Z-score was an exploratory endpoint used to measure the reduction in BMI in children. A clinically significant reduction is generally considered a ≥0.2 reduction in BMI Z-score. A 0.2 reduction is comparable to weight loss of approximately 5%.1,2
Patients were not required to change their diet or exercise routine1
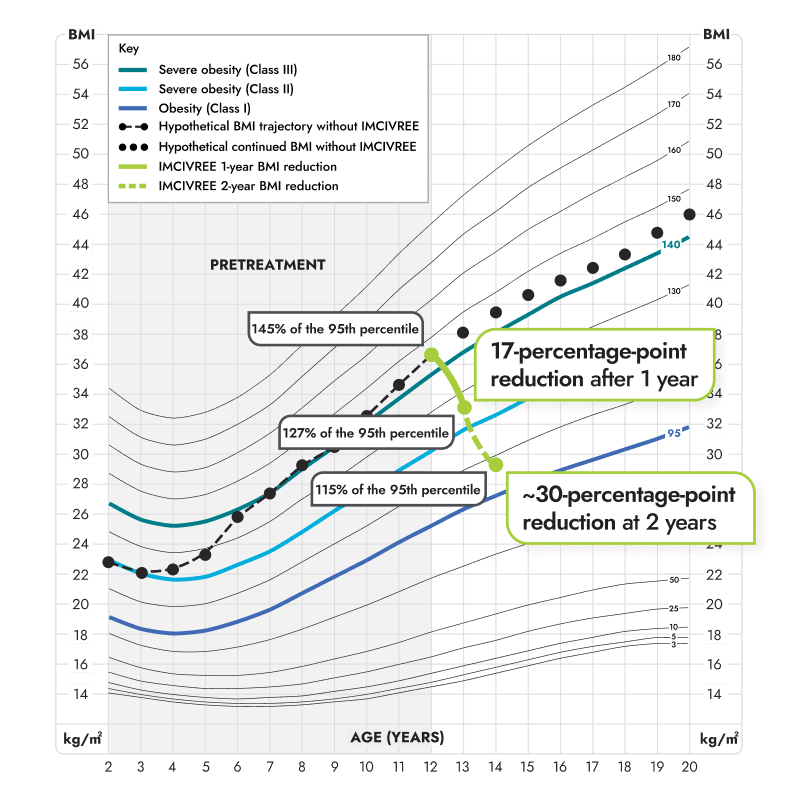
Figure modeled after Gulati AK, Kaplan DW, Daniels SR. Clinical tracking of severely obese children: a new growth chart. Pediatrics. 2012;130(6):1136-1140.6
*Growth chart is based on females 2 to 20 years of age and is for illustrative purposes only.6
In patients ≥12 years of age with BBS
Hunger scores in the 14-week placebo-controlled and 52-week open-label periods1,7*

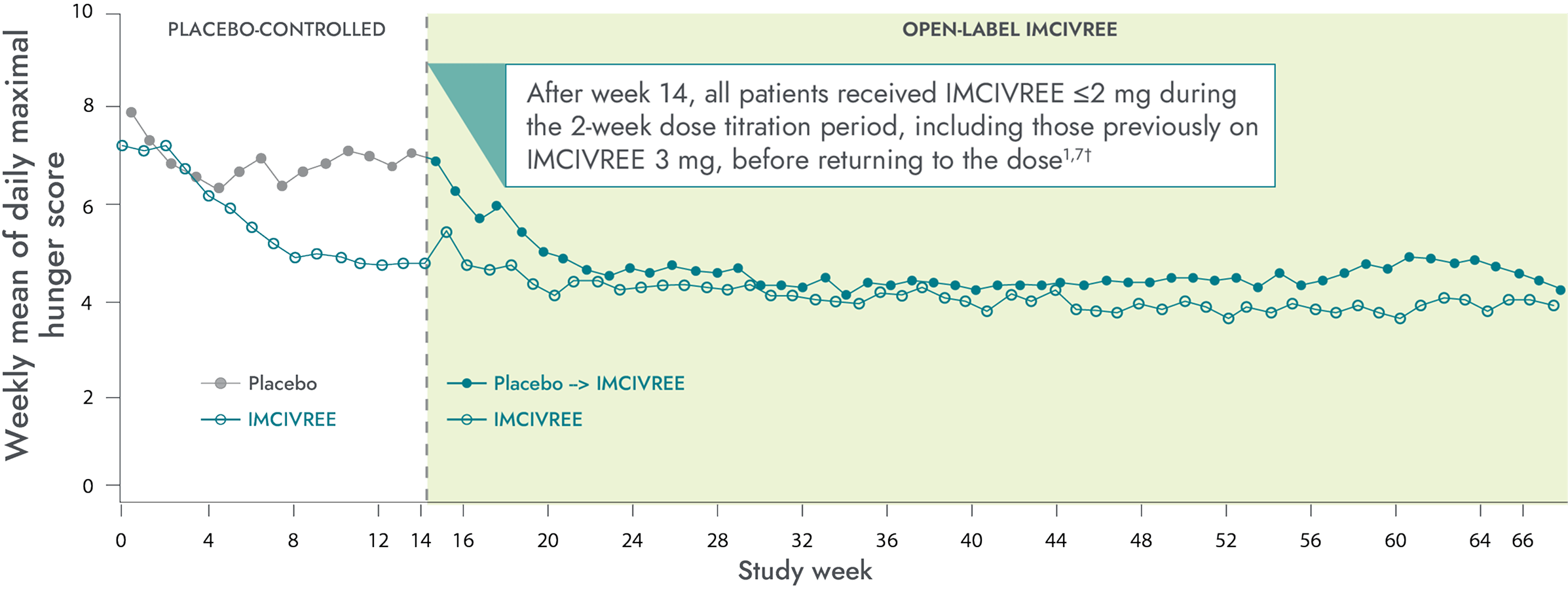
Patients who switched from placebo to IMCIVREE experienced a rapid reduction in hunger, matching that of patients initially assigned to IMCIVREE8
Hunger scale in the BBS clinical trial1
- Patients ≥12 years of age who were able to self-report their hunger (n=14) recorded their daily maximal hunger in a diary, which was then assessed by the Daily Hunger Questionnaire Item 2
- Hunger was scored on an 11-point scale from 0 (“not hungry at all”) to 10 (“hungriest possible”)
Reference: 1. IMCIVREE [prescribing information]. Boston, MA. Rhythm Pharmaceuticals, Inc.
Caregiver assessments were also collected for children <12 with obesity due to BBS‡9
*Patients ≥12 years of age who were able to self-report their hunger (n=14) recorded their daily maximal hunger in a diary, which was then assessed by the Daily Hunger Questionnaire Item 2. Hunger was scored on an 11-point scale from 0 (“not hungry at all”) to 10 (“hungriest possible”).7
†During the placebo-controlled period, dose titration to a fixed dose of IMCIVREE 3 mg given subcutaneously once daily was performed during the first 2 weeks of both the placebo-controlled and open-label periods to maintain blinding.7
‡Data not shown.

The change in Reed’s hunger has cascaded into many positive life changes for all of us. There's less agitation and anxiety over hunger or family meals. This is simple normalcy for many families, but for us, they’re moments I’ll never take for granted.
— Kat, caregiver of a child living with BBS

He is no longer digging through the fridge or garbage, so we do not lock them anymore. He isn’t asking for food constantly between meals and snacks, and I sometimes find myself realizing it’s been a few hours and asking him if he’s ready for a snack.
— Rachel, caregiver of a child living with BBS

Patients and families living with BBS often express such gratitude and relief when started on IMCIVREE and see the weight trajectories and hyperphagia start to improve. To have a medication that can support correcting the biology that is dysregulated and to see positive outcomes provides hope.
— Alaina Vidmar, Pediatric Endocrinologist

These are patients that nothing else has ever worked. So to see them so happy about having something that's finally helping is amazing. Now all they talk about is, ’I'm not hungry all the time. I'm not seeking out food all the time. I'm able to do other things.‘ That shift from the number on the scale to the quality of life, I really love that.
— Christy Davis, Obesity and Weight Management Specialist
Individual results may vary.
Patient-Reported Health-Related Quality of Life
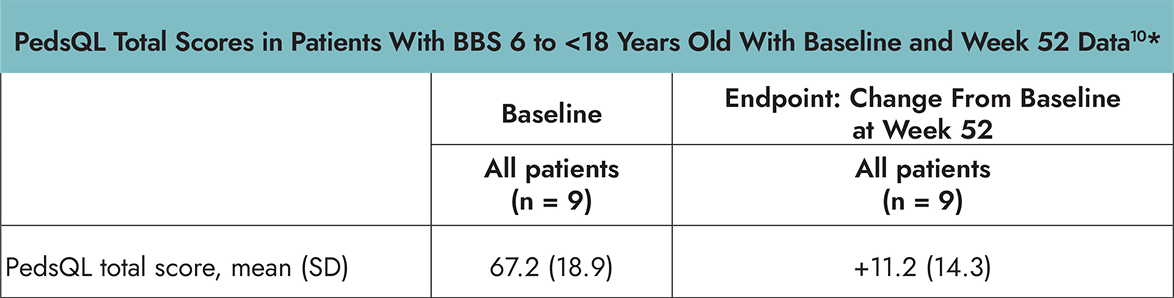
In the Phase 3 trial in patients 6 years and older with BBS, PedsQL and IWQOL-Lite were assessed as exploratory endpoints and were not powered for formal statistical testing or significance. Change from baseline after approximately 52 weeks of treatment was measured by the age-specific PedsQL or IWQOL-Lite assessments.10
- The PedsQL is a 23-item, self-reported, age-dependent assessment of health-related quality of life (HRQOL) in children and adolescents with or without acute or chronic health conditions that encompasses 4 domain scores: physical, emotional, social, and school functioning. The total score is the mean score of the transformed items across the 4 domains. The PedsQL was administered to children 6 to <18 years of age.10,11
- The Impact of Weight on Quality of Life (IWQOL)-Lite is a validated 31-item, self-reported, obesity specific, quality of life questionnaire that provides a total score inclusive of 5 domains: physical function, self-esteem, sexual life, public distress, and work. The IWQOL-Lite was administered to patients ≥18 years of age.10
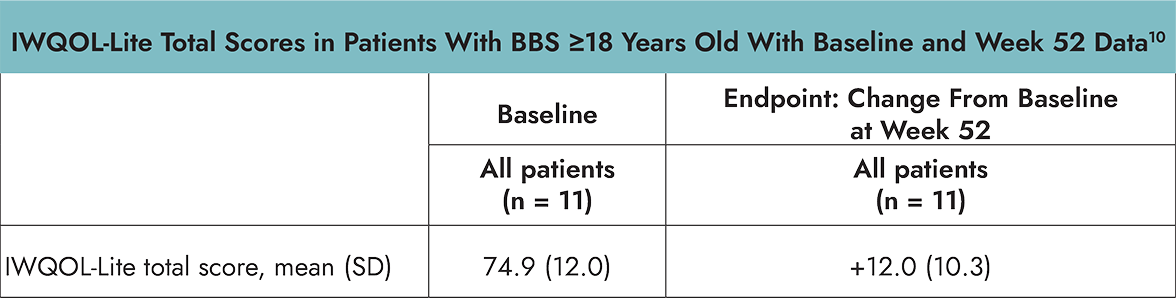
- Raw scores for both PedsQL and IWQOL-Lite were transformed on a scale of 0–100, with 0 representing the worst possible and 100 the best possible HRQOL.10
- Limitations of these results include small sample sizes across assessments, which may be in part due to the rarity of the disease.10
These insights highlight the need to address hyperphagia and subsequent impaired quality of life for people with BBS and their caregivers12
*Using age-specific PedsQL or IWQOL-Lite assessments.10
HRQoL=health-related quality of life; IWQOL-Lite=Impact of Weight on Quality of Life-Lite; PedsQL=Pediatric Quality of Life Inventory.
The impact of IMCIVREE
Hear from families and clinicians about how IMCIVREE is bringing hope for people living with BBS

HRQoL=health-related quality of life; IWQOL-Lite=Impact of Weight on Quality of Life-Lite; PedsQL=Pediatric Quality of Life Inventory.


References: 1. Haqq AM, Chung WK, Dollfus H, et al. Efficacy and safety of setmelanotide, a melanocortin-4 receptor agonist, in patients with Bardet-Biedl syndrome and Alström syndrome: a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial with an open-label period. Lancet Diabetes Endocrinol. 2022;10(12):859-868. doi:10.1016/S2213-8587(22)00277-7. 2. US Preventive Services Task Force, Grossman DC, Bibbins-Domingo K, et al. Screening for Obesity in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA. 2017;317(23):2417-2426. doi:10.1001/jama.2017.6803. 3. Data on file. Rhythm Pharmaceuticals, Inc. Boston, MA. 4. Argente J et al. Endocrine Society Annual Meeting. Poster ODP606. June 11-14, 2022. 5. Data file for the CDC Extended BMI-for-Age Growth Charts. www.cdc.gov. Published December 14, 2022. Accessed January 15, 2025. https://www.cdc.gov/growthcharts/extended-bmi-data-files.htm. 6. Gulati AK, Kaplan DW, Daniels SR. Clinical tracking of severely obese children: a new growth chart. Pediatrics. 2012;130(6):1136-1140. doi:10.1542/peds.2012-0596. 7. IMCIVREE [prescribing Information]. Boston, MA. Rhythm Pharmaceuticals, Inc. 8.Data on file. Rhythm Pharmaceuticals, Inc. Boston, MA 9. Argente J et al. Lancet Diabetes Endocrinol. 2025;13(1):29-37. doi:10.1016/ S2213-8587(24)00273-0. 10. Forsythe E, Haws RM, Argente J, et al. Quality of life improvements following one year of setmelanotide in children and adult patients with Bardet-Biedl syndrome: phase 3 trial results. Orphanet J Rare Dis. 2023;18(1):12. Published 2023 Jan 16. doi:10.1186/s13023-022-02602-4. 11. Varni JW. Scaling and scoring for the acute and standard versions of the Pediatric Quality of Life Inventory™ PedsQL™. Version 21.3. March 2023. Accessed December 15, 2024. https://www.pedsql.org/PedsQL-Scoring.pdf. 12. Eneli I, Xu J, Webster M, et al. Tracing the effect of the melanocortin-4 receptor pathway in obesity: study design and methodology of the TEMPO registry. Appl Clin Genet. 2019;12:87-93. doi:10.2147/TACG.S199092.